Cadence and (micro) managing Type 1 Diabetes to create Ease from dis-ease
By JC
Abstract
This article describes a personal journey of how to live well with Insulin Dependent Diabetes Mellitus (IDDM), i.e., Type 1 Diabetes, using “three-axis” control (two or three-axis control also benefits Type 2 Diabetes management). A historical perspective is given from the discovery of insulin to the level of blood glucose (BG) control possible today — transforming dis-ease into comparative ease. The ongoing study, beginning in 2016 through the present, was to determine if non-diabetic HGBA1c can be safely approached and sustained, over a long term, while avoiding hypoglycemic episodes.
The study subject, a Type 1 Diabetic (T1D) of over 6 decade duration (61st year in 2025), was fitted with 1) Dexcom G5 and later G6 Continuous Glucose Monitor (CGM), 2) Animas insulin pump and later Tandem t:slim X2 pump, and 3) iPhone with Apple Watch (Series 2, Series 5, Series 9). All CGMs were fasting calibrated following each replacement using OneTouch BG test strips.
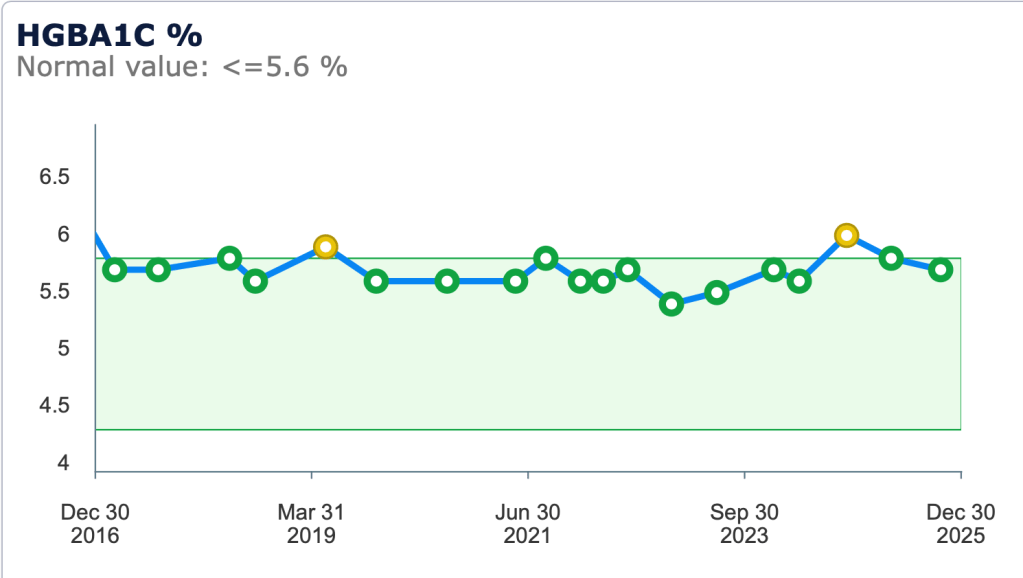
To address the root problem of maintaining non-diabetic BG without hypoglycemia, the study subject T1D took into account “insulin demand” variations and practiced three-axis control (insulin, food, physical activity) employing mindful choices through a process of trial and error learning to find “a range of cadences that work…” to achieve BG control. During the ongoing 9 year study, HGBA1c range from 5.4% to 5.9% (5.7% average) without hypoglycemia.
Today’s CGMs allow monitoring BG in almost real time (allow for lag between CGM interstitial fluid glucose reading and real blood glucose) to safely maintain BG approaching non-diabetic HGBA1c in the mid to high fives, while avoiding hypoglycemic episodes — if the T1D strives to mindfully use three-axis control.
Cadence
There is cadence in many aspects of life. Cadence is the measure of something rhythmic and balanced and it can be sensed if we are mindful and patient. We can feel, hear, or see cadence all around us — in nature, music, speech, dance, poetry, military march, skating, and cycling. Amanda Gorman’s inaugural recitation of her poem, The Hill We Climb, is a powerful example of cadence. Cadence, with a trial and error faltering start, is beautifully depicted by Deborah Kerr and Yul Brynner in the Shall We Dance scene in the 1956 musical film, The King and I. (See videos at the end of this article.)
Each one of us is different but each one of us can develop our own cadences for life with mindful effort and learning by trial and error.
Experience…matters, and [bicycle] riders who have logged lots of miles…will likely have found a range of cadences that work for them, depending on the terrain and demands of a particular ride.1
As in riding a bicycle, you must balance, steer, and pedal before life takes you anywhere. But without cadence, it’s not enough to go far — whether or not you have Type 1 Diabetes (T1D).2
History
2021 marked the centenary of Dr. Frederick Banting’s surgical extraction of canine insulin that began on the night of October 31, 1920 at 2 a.m. while, “unable to sleep…thinking…, had an idea and wrote a note to himself” in his notebook:
Ligate pancreatic ducts of dog. Keep dogs alive till acini degenerate leaving Islets. Try to isolate the internal secretion of these to relieve glycosurea.3, 4
Banting’s surgical insight* to preserve the internal secretion of the pancreas (insulin) set the stage for the future of diabetes treatment and forever changed the diabetes Death Sentence to Life — a Life Sentence of mindfully managing and balancing multiple daily insulin injections, diet, and exercise plus testing, monitoring, and adapting to minimize episodes of hypoglycemia, insulin shock (seizure), or hyperglycemia and diabetic ketoacidosis.
In July 1921 the extracted insulin lowered the blood glucose of a diabetic dog. Subsequently, bovine insulin from slaughterhouses was purified and administered to the first diabetic patient in January 1922. Before this, diabetes was a fatal disease and diabetics were placed on a starvation diet, wasting away, while family prayed and waited for their inevitable passing. One can only imagine what this was like for the families and patients — progressive weight loss, polyuria, and thirst, leading to eventual diabetic ketoacidosis and death. Dr. Frank Allan, who was a senior medical student in 1921 recounts, during a talk given in 1971, seeing Leonard Thompson prior to him becoming the first patient treated with insulin.5
…a fourteen-year-old boy…admitted to Ward H of the Toronto General Hospital in December 1921. He had been diabetic for approximately two years and although dietary treatment had been attempted, he had been failing steadily in health. He was admitted to the hospital in a serious condition, emaciated and feble. The dietary regimen employed in the hospital failed to check his downward course. He was a pathetic figure as he lay quietly in his bed or sat still in the chair at the bedside, too weak to show interest in the activities of the large, busy ward. All of us knew that he was doomed.5
The sobering descriptions of life and death before insulin are a reminder of how fortunate we are today with the tools we have to not only manage diabetes but to live an active, creative, productive, long, and healthy life.5, 6
* The surgical technique was later found to be unnecessary but “Banting’s great idea…had been useful…to start the Toronto research.” Charles Best assisted Banting and worked on purifying the “internal secretion”. Purification was refined by James Collip for use on human patients. Peter Maloney further refined the process for large scale production. The work was done in the laboratory of J.J.R. Macleod based on Banting’s notebook proposal — their first meeting was on November 7, 1920.3, 4

Finding and Maintaining the Balance
As a 9th grader in 1965, 44 years after Banting’s success, I vividly recall Dr. Fred Whitehouse (1926-2019), Division Head of Metabolic Diseases, Henry Ford Hospital, pulling up a chair and having me sit next to him at his office desk as he described “that dumb insulin” while he drew absorption curve graphs of long acting Neutral Protamine Hagedorn (NPH) and quick acting Regular insulin so I could visualize the timing and absorption of my daily insulin injections. The insulin was “dumb” because once injected, you were committed, and responsible to eat on time to keep blood glucose from going to dangerous, and possibly deadly, lows. He said that I would have to know more about my body than he could ever know. He also stressed the importance of timing with respect to insulin injections and meals i.e., keeping them on schedule and balanced. The daily injections kept me alive, I regained lost weight, and flourished. In those days, home blood glucose tests, let alone multiple daily tests, or the glycohemoglobin test, HGBA1c (average blood glucose for three preceding months), did not exist. Managing was a challenge without respite.
Non-diabetics eat food and their pancreas will provide insulin to match the food. Type 1 diabetics do the reverse. They must first take exogenous insulin, followed by mindful food choices to match the insulin. It’s that simple. But the implementation of a simple solution is often complicated…
Technical Help
Initially, the only home testing that could be done was checking for glucose and ketones in urine. Their presence indicated that blood glucose had already gone too high or exceedingly high. But things did improve and each step eased the way. When I first gained access to disposable insulin syringes I was elated because I didn’t have to daily sterilize (by boiling) a glass syringe and needle (sharpening the latter with a honing stone). Fourteen years after diagnosis, I was able to test blood glucose occasionally with an analog reflectance colorimeter. By the late 1980’s digital glucose meters became available for multiple daily blood glucose tests that provided a more detailed view of glucose variations. The daily injections continued for 39 years until I switched to my first insulin pump in 2004.
Three-Axis Control – Learning by Trial and Error
The story of the Wright brothers’ struggles to fly and their progress of repeated cycles of failure, learning, and acting on their learning from 1899 to 1905, are inspiring to me as a T1D because it parallels what we do to learn BG control i.e., learning takes patience, effort, and time. Lacking formal training, the Wright brothers began their quest to fly using their knowledge of riding and balancing bicycles, and they repaired and built bicycles to fund their flight experiments. They started with gliders, at first only trying to glide in a straight line, gradually increasing distance, and began crude attempts to steer. As their experiments and testing progressed, they came to see and understand the three-axis control required for flight. They perfected control mechanisms through trial and error learning, and acting on their learning. Their three-axis flight control system (roll, pitch, and yaw) remains unchanged but has refinements and technological enhancements to assist the pilot.7
The three-axis control for Type 1 diabetes management are: insulin, diet, and exercise. And today, we have refinements and technological enhancements. The two-axis control of non-insulin dependent Type 2 diabetes management are diet and exercise.
Insulin is now manufactured using recombinant DNA technology and available without relying on limited animal extracts. Diet and food preparation guidance are available through consultation with a Registered Dietician (RD) working in concert with your health care team. The Diabetic Exchange8, 9 list is the way I learned about food — what to eat and how much, along with scheduled timing of meals and snacks. Measure what you eat and learn about carbohydrate counting (and its correlation to insulin), glycemic index, protein, and fat. Be in control and prepare your own foods so you can eliminate unknown excess fat, oil, grease (FOG) and sugar — reduce these by at least 50% to 75% in any recipe. Avoid all fried foods and choose grilled instead. Stay heart healthy, follow a plant based diet and reduce or eliminate meat. Poultry and fish should be grilled (not fried). A good reference for learning is The CalorieKing Calorie Fat & Carbohydrate Counter.10 Exercise should be consistent and can take many forms. My favorite is a daily outdoor bike ride.
Just as the pilot must pay attention and remain in control of each axis for a successful flight, a diabetic must pay attention and remain in control of each axis for successful management.
Solution to Problem should be Sought at its Root
On the occasion of receiving an honorary doctorate degree in the spring of 1974 at Michigan Technological University, Soichiro Honda (also with a bicycle mender background) said:
Many people dream of and hope for success. To me, success can be achieved only through repeated failure and introspection. …final success can only be achieved if you face challenges. …the solution to any problem should be sought at its very root.11
Faced with the vehicle emissions standards of the Clean Air Act required by 1975, rather than complaining and pushing back as some manufacturers (are you pushing back and complaining instead of managing your diabetes?), Mr. Honda guided his team to go to the root problem—the combustion process—resulting in the Compound Vortex Controlled Combustion (CVCC) engine system that’s still in use today.11
The root problem of Type 1 diabetes, lack of insulin, has been solved with exogenous insulin.
The root problem of Type 1 diabetes management, maintaining blood glucose within normal levels (as much as possible), can be managed through trial and error learning, and acting on that learning. Managing our blood glucose efficiently using three-axis control is managing our internal combustion process.
The benefits of keeping blood glucose within normal levels was confirmed in the Diabetes Control and Complications Trial (DCCT) between 1983-1993.
The DCCT showed that people with type 1 diabetes who kept their blood glucose levels as close to normal as safely possible with intensive diabetes treatment as early as possible in their disease had fewer diabetes-related health problems after 6.5 years, compared with people who used the conventional treatment.12
DCCT participants who had tight control of their blood glucose levels had a 33 percent lower risk of death, 21 years after the DCCT ended. Historically, people with type 1 diabetes tended to die earlier than the general population. DCCT/EDIC researchers found that this earlier death can be reduced through careful management of blood glucose.12
More Technical Help allowing Micro-Management
For years, I have used the Dexcom Continuous Glucose Monitor (CGM), Apple Watch, and Tandem t:slim X2 insulin pump (another three-axis control). The CGM transmits blood glucose via Bluetooth to my iPhone and the phone to Apple Watch. A quick glance at my watch reveals blood glucose and trends (increasing, decreasing, or level) and gives warnings if blood glucose is outside set thresholds. The pump and CGM can also be set up as a loop but I’ve chosen not to use the feature because no algorithm can know in advance how physically active I may be during the day e.g., a 5 or 35 km bike ride. Being able to see blood glucose and trends on my watch allows immediate adjustments (micro-management) when needed just as easily as changing gears on the bicycle. Unlike the past, when I could only crudely measure insulin in 1U increments with a syringe, the pump can accurately deliver as little as 0.05U.
Balance, Steer, and Pedal with Cadence
My approach to the root problem of Type 1 diabetes management (blood glucose control) is similar to what I do when riding my multi-gear bike to maintain pedaling cadence — I anticipate and make the gear changes just before they are required. If you don’t ride a multi-gear bicycle, read about cadence and see how it parallels our control efforts.13 The bike crankset, sprocket(s) at the pedals, is akin to the basal insulin dose delivered by the pump. The basal dose is a steady delivery of quick acting insulin throughout the day. When I have a meal, the basal dose is supplemented by a bolus dose of insulin to account for the meal. The bolus is akin to the gear cluster controlled by the bike’s rear derailleur. Riding the bike, I’ll change gears at the crankset and/or derailleur depending on the ride e.g., ascent, descent, level, difficult terrain, strong headwind, tailwind, and distance, in order to maintain pedaling cadence without undue strain.
Just as the key to maintaining pedaling cadence on a bike ride begins with selecting the best sprocket at the crankset for the conditions, the key to successfully managing T1D is selecting the best basal dose for the conditions.
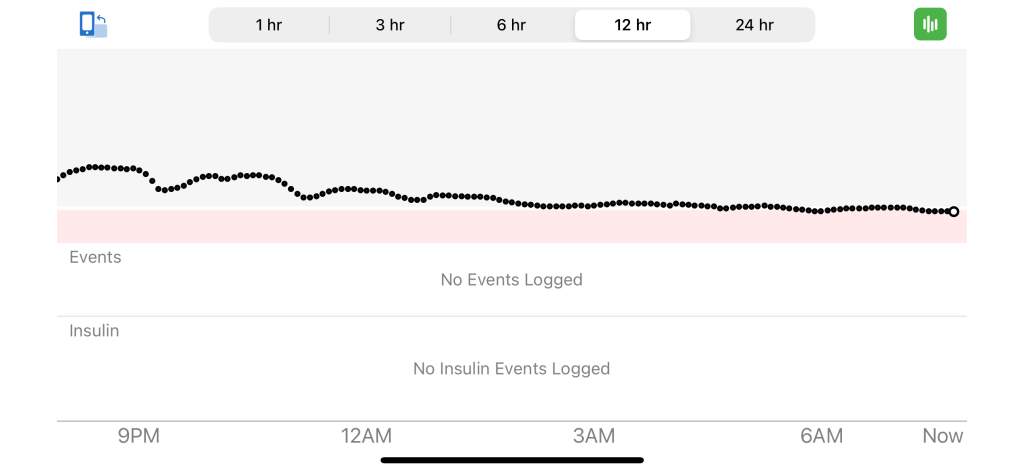
The basal setting of the pump allows creation of multiple basal profiles. I use a high setting for a sedentary day, a low setting for sleep, and other settings in between for varying levels of physical activity — this is like selecting a sprocket at the crankset. The bolus insulin dose taken with meals, or to lower a high blood glucose, varies with the meal carbohydrates or elevated blood glucose. My sleep “equilibrium” basal rate is 37.5% of my sedentary day basal rate (see graph below). The higher sedentary day basal rate blunts the glucose rise from meals resulting in less bolus — reducing/eliminating hypoglycemia drama.
For those wondering why you need more insulin when sedentary (not moving, sitting at a desk but having meals), watch the educational (self-discipline) and entertaining kitchen caution, “The Fridge Again” by talented gospel singer, KD French, as she does all the choir voices (see video at the end of this article). Her wise counsel was created during the COVID lock down and will benefit Type 1 and Type 2 diabetics.
Learning by trial and error, and making small changes, one can determine (with your health care team) the following values (bolus dose must take into account basal dose):
a) What is the basal rate of insulin that keeps your blood glucose flat and steady without food, for example at 80mg/dL (it can be higher at 110mg/dL as you begin learning)? This “equilibrium” setting is used for sleep to avoid hypoglycemia (low blood glucose).
b) What is the bolus dose of insulin required for a meal or snack with 20gm carbohydrate?
c) What is the bolus dose of insulin required to lower your blood glucose by 50mg/dL?
These values will change as you grow or if you are stressed (see more discussion below) or anxious. BG rise requiring more insulin can also be due to intense physical activity (“…epinephrine is an important contributor to stress-induced hyperglycemia….”14, 15), receiving a vaccine, a common cold or other illness, a stressful drive in heavy traffic, meeting a deadline for school, work, or preparing for an exam. Along with food they create, what I call, insulin demand.** Once you know these values and how they work in your body you can change “gears” as needed in order to micro-manage the root problem of blood glucose control and meet the insulin demand (as it increases, decreases, or remains steady), almost as easily as riding a bike.
Intense physical activity, intermittent or continuous, will result in elevated glucose requiring more insulin. “Epinephrine-induced hyperglycemia is markedly accentuated by concomitant elevations of glucagon and cortisol or in patients with diabetes. In both cases, the effect of epinephrine on hepatic glucose production is converted from a transient to a sustained response, thereby accounting for the exaggerated hyperglycemia.”14 To turn this “sustained response” off, you must add insulin. If your activity is such that you can’t carry on a normal conversion, it’s likely you reached 80% max VO2 and you can expect the elevated glucose to begin.15
The “Impact of stress” on control efforts must be recognized, and can be mitigated. “Chronic stress can produce basically all the so called chronic noncommunicable disorders including obesity, metabolic syndrome, diabetes Type 2, hypertension, depression, anxiety, and so on.” See the video at the end of this article: Impact of stress — an interview with Prof. George P. Chrousos MD ScD. He currently holds the UNESCO Chair on Adolescent Health Care.
The Nature Prescription is one way to reduce and/or eliminate stress. Being physically active (daily if possible) e.g., walk, hike, bike ride, swim, ski, skate, ballroom dancing, etc., provide a “nature prescription”. Listening to good tunes can help you out of the “diabetic doldrums” (see video Hang on Little Tomato by Pink Martini/China Forbes at the end of this article).
The Nature Prescription
Tips or Tricks?
There are none. The notion that there are short cuts to managing Type 1 or Type 2 in my view is a disservice. There is no medication or device that absolves the diabetic from making daily mindful choices about food and physical activity. Non-diabetics are also not absolved from making mindful choices about food and physical activity if they seek long term good health. CGMs and pumps, as good as they are in providing flexibility and freedom, do not relieve a diabetic from mindful choices, but eliminate the tedium of multiple daily blood glucose tests and injections.
An unsung benefit of the control possible with the sensor, pump, and watch, is that you can avoid or limit feeding “that dumb insulin” due to hypoglycemia. “The short- and long-term complications of diabetes related hypoglycemia include precipitation of acute cerebrovascular disease, myocardial infarction [heart attack], neurocognitive dysfunction, retinal cell death and loss of vision in addition to health-related quality of life issues pertaining to sleep, driving, employment, recreational activities involving exercise and travel.”16
If you don’t use a pump but take a long acting insulin and multiple daily injections (MDI), it’s similar to riding a bike with one sprocket at the crankset but you still use a rear derailleur for multiple bolus doses of quick acting insulin for meals or elevated blood glucose. British comedian Ed Gamble provides a humorous description of this process. https://streamable.com/kuyoj8.
The benefits of managing basal rates, as I do to match my activities and meals, has been known for decades and was described in 2002, Diabetes management in the new millennium using insulin pump therapy: “In comparison to multiple daily injections (MDI), … [pump therapy] uses only rapid-acting insulin, provides greater flexibility in timing of meals and snacks, has programmable basal rates to optimize overnight glycemic control, can reduce the risk of exercise-induced hypoglycemia, and enhances patients’ ability to control their own diabetes. Most important, in adults and adolescents with type 1 diabetes, … [pump therapy] has been shown to lower …[HGBA1c] levels, reduce the frequency of severe hypoglycemia and limit excessive weight gain versus MDI without increasing the risk of diabetic ketoacidosis.”17
If you are helping a young child, there are useful books but one of my favorites, because it’s concise and shares the ups and downs from a child’s perspective: Nothing can stop me with T1D! 9798663865883: Amazon.com: Books https://a.co/d/aDTjkai. The author was diagnosed age 5, began pumping insulin age 5, published her book age 14, and is now in medical school!
** Pumpers are familiar with the term “correction factor” as it’s used for making insulin dose adjustments due to high blood glucose or carbs. I’ve never liked the term because it’s negative, implying that you, the T1D, have made an error needing correction. My term “insulin demand” is a better description of what’s going on — your body is asking for more or less insulin because it’s needed.
Diabetes is a Responsibility, just like any other
At the outset of my diabetes journey I learned from diabetic Davis Cup tennis champion, Bill Talbert, as described in his book Playing for Life, that “Diabetes is a responsibility, just like any other.” In other words, it’s a job that requires tasks to be done, done well, and done on time. I understood Responsibility because I delivered daily newspapers on bicycle before diagnosis, and after one month in hospital, continued the job after diagnosis.
Bill Talbert was diagnosed at age 10 in 1928, and began playing tennis at age 14. He completed 70 laps around the sun as Type 1. I was diagnosed age 13, began playing tennis at age 14 and now on my 61st lap around the sun as Type 1. Lacking today’s control tools my early years were not easy but the advice of another tennis great, Arthur Ashe, kept me reassessing. “Start where you are, Use what you have, Do what you can“. He was talking about tennis, but the wisdom applies to any undertaking and, for me, that includes managing diabetes. “Bring thyself to account each day…” and take small steps to make it better. Nearly everyone I’ve met that was struggling with diabetes, both Type 1 and Type 2, had common issues having to do with food and lack of physical activity. We are continually marketed processed, rich, refined, and fried [non] foods. These may have a high glycemic index causing a steep glucose rise that can’t be matched by insulin absorption and may continue to elevate BG for an extended time. This results in the never ending “roller coaster” (glucose swings between high and low) as you administer bolus.
Bill Talbert developed his aggressive net game to lessen running back and forth on the backcourt to limit hypoglycemia. This strategy, born out of being a “juvenile onset insulin dependent diabetic” (aka Type 1), contributed to his many wins.
Tight Control to the Flame of Hope
Anyone wanting to stay healthy makes mindful food choices, engages in at least a modest exercise regime, and sleeps and eats on schedule. Diabetics should do all these things, plus add insulin and monitor blood glucose i.e., they are their pancreas. And you’ll need patience, with yourself and others, on this life long journey. Rather than viewing diabetes as a management struggle, it can be eased with the choices we make, using available tools so it becomes as intuitive as balancing and riding a bicycle — trial, error, and learning. Like riding a bike, it may be difficult at first but once learned, it’s easy. The tight control that can be achieved using the Dexcom CGM, Apple Watch, and Tandem pump, were unimaginable a few years ago. Compared to what I faced as a 9th grader, when I could only guess what my blood glucose had been (based on a urine test), today’s tools allow me to see my blood glucose in (almost) real time18 and where it’s going. Instead of looking back to what had been, I can now look forward to what will be.
Wayne Gretzky, one of the greatest hockey players of all time, summarizes this approach. “A good hockey player plays where the puck is. A great hockey player plays where the puck is going to be.”
By learning through trial and error, it’s easy to approach non-diabetic blood glucose control. My glycohemoglobin, HGBA1c, over the past eight years range from 5.4% to 5.9% with an average of 5.7% without hypoglycemia. Note the high value in 2024, see graph below, was due to denatured insulin.
Managing basal rates empowers you to transform what Dr. Whitehouse described as “that dumb insulin”, to insulin that is “smart” and matches what you are doing without hypoglycemia.
The thoughtful choices we make now will contribute to our longevity so that one day we’ll see the Flame of Hope goal finally realized:
“The Flame of Hope is an eternal flame [kindled in 1989] that honours Sir Frederick Banting’s discovery of insulin as well as all those who have been affected by diabetes located in London, Ontario, Canada. Simultaneously, it serves as a reminder that insulin manages diabetes but does not cure it; ultimately, it stands for the hope that a cure will soon be found.
The Flame will only be extinguished when a cure for diabetes is developed.”19
Words of Wisdom for Diabetics: “…they knew what they should do themselves.”
“In a 2012 interview Dr. Whitehouse stated his belief that the next leap forward…. [I]n my view will come the ‘cure of the insulin-dependent diabetic person.’ This will require stem cells from the diabetic’s own tissues developing into beta cells, then preventing these ‘personal’ beta cells from being killed off as they initially were. This will be the crowning achievement. That’s all coming….”.20, 21
On November 16, 2021 “Canada’s medical agency Health Canada…approved… [Phase 1] clinical trial application for VCTX210, a CRISPR-edited stem cell therapy designed to treat type 1 diabetes [and insulin dependent type 2]. This is a milestone in medicine as it marks the first ever gene-edited therapy for diabetes to approach the clinic. …[And] is engineered to evade the immune response…, which also eliminates the requirement for immune suppression therapy.”22, 23, 24 Note the timing and place of this announcement — the centenary of Banting’s insulin discovery and the start of Phase 1 clinical trial in Canada.
“On March 9, 2023, Vertex Pharmaceuticals received FDA clearance to begin human trials with a new stem cell therapy, VX-264. VX-264 involves surgically implanting a protective device containing insulin-producing stem cells into the body of a person with type 1 diabetes (T1D) without the need for immunosuppression.”25
“When Fred [Whitehouse] was asked ‘What do you want your patients to remember about you?’ he answered: ‘…I would hope that they would think that I was trying my best to help them. But that I also was not doing it for them, but they knew what they should do themselves. …I would hope that people, when it comes to diabetes, would say to themselves Well I can, I can do better because he helped me do better’ [my emphasis].
Dr. Fred W. Whitehouse was a gentleman who made an incredible impact on treating diabetes for more than seven decades.”20
2. https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/type-1-diabetes
3. https://www.thecanadianencyclopedia.ca/en/article/the-discovery-of-insulin
4. https://academic.oup.com/clinchem/article/48/12/2270/5642437
5. Allan, F. (1972). DIABETES BEFORE AND AFTER INSULIN. Medical History, 16(3), 266-273. doi:10.1017/S0025727300017750 (Presented at the Annual Symposium of the New England Diabetes Association, on 13 November 1971 is available here via search as a pdf: https://www.cambridge.org/core/services)
6. https://insulin.library.utoronto.ca/about/patients
7. https://en.wikipedia.org/wiki/Wright_brothers
8. http://www.diabetesed.net/page/_files/THE-DIABETIC-EXCHANGE-LIST.pdf
9. https://www.tasteofhome.com/article/diabetic-exchanges/
10. Borushek, Allan, 2010. The CalorieKing Calorie Fat & Carbohydrate Counter. Costa Mesa: Family Health Publications
11. Sanders, Sol. 1975. Honda: The Man and His Machines. Boston: Little, Brown and Co., p. 10.
13. https://sheldonbrown.com/gears.html,
14. https://pubmed.ncbi.nlm.nih.gov/6380304/
15. https://www.diabeteshealth.com/exercise-often-raises-blood-glucose-in-type-1-diabetes/
16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3784865/
17. https://pubmed.ncbi.nlm.nih.gov/11921425/
18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8245065/
19. https://en.wikipedia.org/wiki/Flame_of_Hope_(diabetes)
20. https://care.diabetesjournals.org/content/42/12/2167
21. https://www.healthline.com/diabetesmine/meet-dr-whitehouse-historical-endo-extraordinaire#1
23. https://diatribe.org/viacyte-and-crispr-introduce-new-stem-cell-therapy-for-type-1-diabetes
About the Author:
JC, johntcT1D@gmail.com, with his 20-speed bike at the base of Wright Brothers Memorial, south of Kitty Hawk, North Carolina, site of the Wright brothers flights. In September 2025, JC completed 74 laps around the sun and was on his 61st lap as Type 1.

Disclaimer: This article is intended to share my journey of learning to live well with diabetes and is not medical advice. Seek guidance and medical advice from your health care provider. Live Long and Prosper (LLAP).
The links below: The Hill We Climb by Amanda Gore, Shall We Dance scene from The King and I musical film, and The Fridge Again!! by KD French.
Hang On Little Tomato by Pink Martini/China Forbes

Thank you… a wonderful read. Your creativity and knowledge made this fascinating and informative.
You are an excellent writer.
LikeLike
As a T1D for 45 years, I thoroughly appreciated and enjoyed your inspiring perspective, wonderful analogies and the videos at the end! I had hit a place of great discouragement with mine and really feel blessed by your article and attitude! We all need this kind of renewal and inspiration in life – not just those of us with type 1, right? Thank you for sharing this article via your Reddit post today. You are a truly uplifting and inspiring person!
LikeLike